NextGen 2024: Refractory SJIA & MAS Session Part 8
 AI Summary
AI Summary
Key Insights
- The document discusses the challenges in treating refractory adult Still's disease, including defining what constitutes 'refractory' and the various treatment options available.
- It explores different phenotypes of adult Still's disease, focusing on clinical heterogeneity and the need for stratification based on the disease's activity level and underlying immune mechanisms.
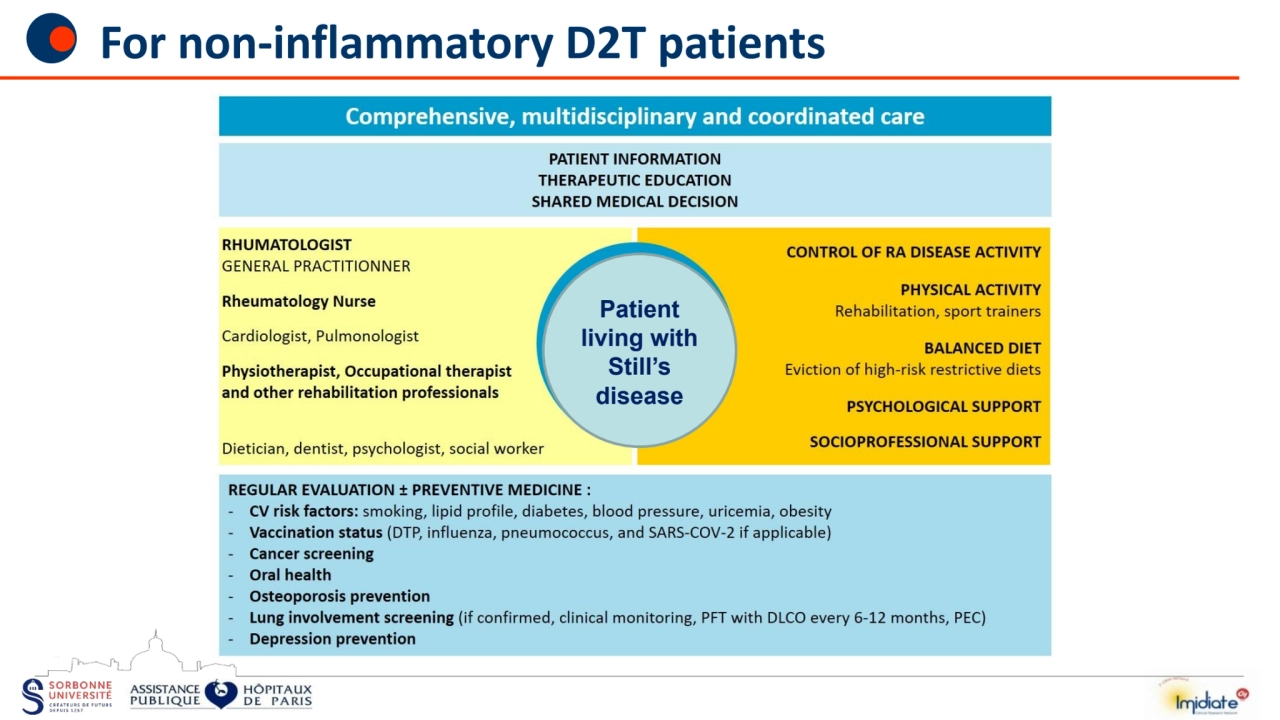
- The content refers to recommendations and strategies for managing non-inflammatory D2T patients and emphasizes comprehensive, multidisciplinary care including patient education, therapeutic interventions, and coordinated medical decision-making.
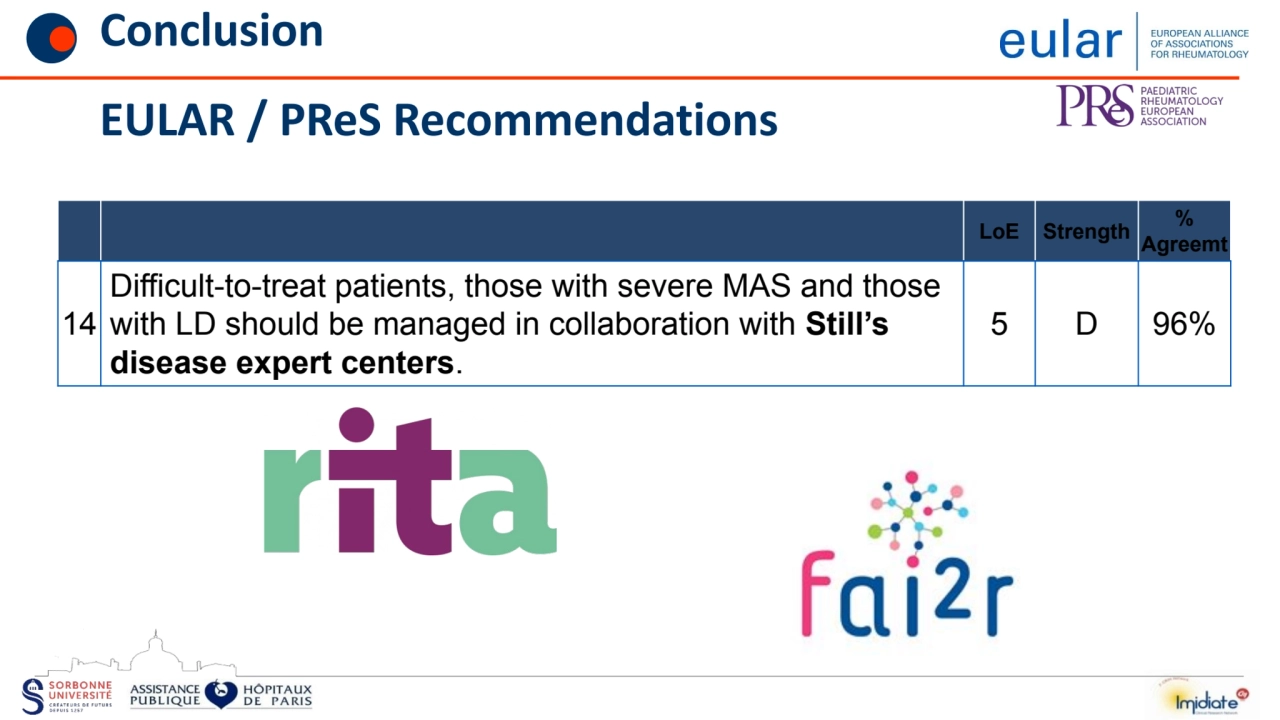
- The document provides insights into the importance of considering hyperinflammatory complications, like Macrophage Activation Syndrome (MAS), and EULAR/PRES recommendations for managing difficult-to-treat patients in specialized expert centers.

![Adult Still's disease (MSA)
• Still's disease in children
– Systemic form of AJI (FS-AJI)
Systemic onset JIA (SoJIA)
– 1
ere description in 1897 by Sir G Still
• Fever + Rash + Arthritis triad
– Evolution by recurrent attacks
• Prevalence 3.1 / 100000 [0.5-0.7]
• Incidence 0.6 / 100,000 [2.7-3.6]
Thierry S, 2011
• Adult form :
– Adult Still's disease
Adult onset Still's Disease (AoSD)
– 1st description by Bywaters in 1971
• Triad: Fever + Rash + Arthralgia/itis
– Recurrent attacks, young adults
• Prevalence: 0.16 to 1.5 / 100,000
Magadur-Joly 1995, Wakai 1997
• No gender predominance
• No family aggregation
• No clear comorbid association](https://d2z384uprhdr6y.cloudfront.net/o14WYegBjK3vrHf5bVoA4aoklCgG36yyxjjUQfzRzRs/rt:fill/q:100/w:1280/h:0/gravity:sm/czM6Ly9qYXVudC1wcm9kdWN0aW9uLXVwbG9hZHMvMjAyNC8xMi8wNS9jZmM4YTgxYi00MWNiLTRiMTktOTMwMy02MGY4NTU0ZGZkZmQvc2xpZGVfMy1sLndlYnA=.webp)
NextGen 2024: Refractory SJIA & MAS Session Part 8
- 1. Treating Refractory Adult Still's Patients Bruno Fautrel, MD PhD Sorbonne University - Assistance Publique Hôpitaux de Paris Rheumatology Department, GH Pitié Salpêtrière CRI - IMIDIATE Clinical Research Network Pierre Louis Institute of Epidemiology and Public Health INSERM UMRS 1136, Team 5
- 2. • Financial interests – None • Permanent links – None • Interventions – AbbVie, Amgen, Biogen, BMS, Celltrion, Fresenius Kabi, Galapagos, Gilead, Janssen, Lilly, Medac, MSD, NORDIC Pharma, Novartis, Pfizer, Roche, Sandoz, Sanofi-Genzyme, SOBI, UCB, Viatris. • Indirect links – Research grants: AbbVie, Lilly, MSD, Pfizer Links of interest
- 3. Adult Still's disease (MSA) • Still's disease in children – Systemic form of AJI (FS-AJI) Systemic onset JIA (SoJIA) – 1 ere description in 1897 by Sir G Still • Fever + Rash + Arthritis triad – Evolution by recurrent attacks • Prevalence 3.1 / 100000 [0.5-0.7] • Incidence 0.6 / 100,000 [2.7-3.6] Thierry S, 2011 • Adult form : – Adult Still's disease Adult onset Still's Disease (AoSD) – 1st description by Bywaters in 1971 • Triad: Fever + Rash + Arthralgia/itis – Recurrent attacks, young adults • Prevalence: 0.16 to 1.5 / 100,000 Magadur-Joly 1995, Wakai 1997 • No gender predominance • No family aggregation • No clear comorbid association
- 4. « Refractory » Adult Still’s Patients • Refractory or « D2T » : lack of definition • Several options – Drug dependency or Inadequate response • Prednisone? Or bDMARD? – Life threatening complications? • MAS, lung disease, fulminant hepatitis – Non-inflammatory residual symptoms • Fatigue, residual pain, consequences of high dose steroids…
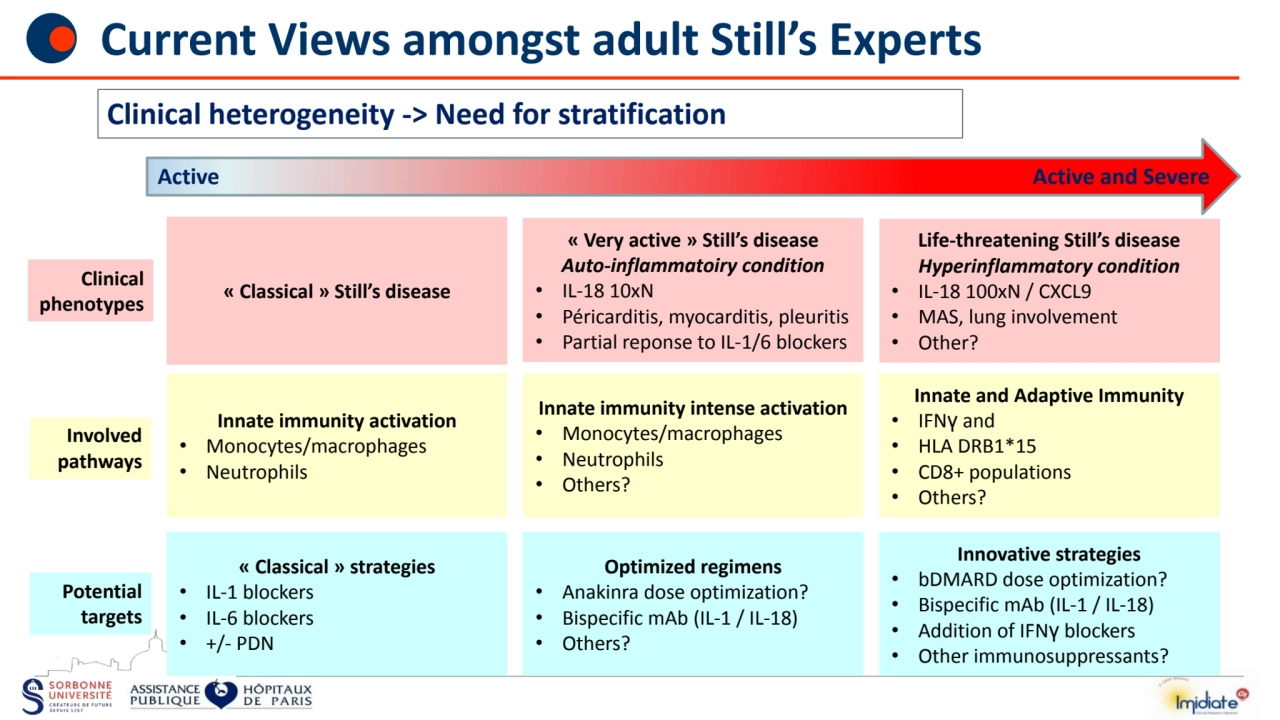
- 5. Active Active and Severe « Very active » Still’s disease Auto-inflammatoiry condition • IL-18 10xN • Péricarditis, myocarditis, pleuritis • Partial reponse to IL-1/6 blockers Life-threatening Still’s disease Hyperinflammatory condition • IL-18 100xN / CXCL9 • MAS, lung involvement • Other? « Classical » Still’s disease Clinical phenotypes Innate immunity activation • Monocytes/macrophages • Neutrophils Innate immunity intense activation • Monocytes/macrophages • Neutrophils • Others? Innate and Adaptive Immunity • IFNγ and • HLA DRB1*15 • CD8+ populations • Others? Involved pathways Clinical heterogeneity -> Need for stratification Current Views amongst adult Still’s Experts « Classical » strategies • IL-1 blockers • IL-6 blockers • +/- PDN Optimized regimens • Anakinra dose optimization? • Bispecific mAb (IL-1 / IL-18) • Others? Innovative strategies • bDMARD dose optimization? • Bispecific mAb (IL-1 / IL-18) • Addition of IFNγ blockers • Other immunosuppressants? Potential targets
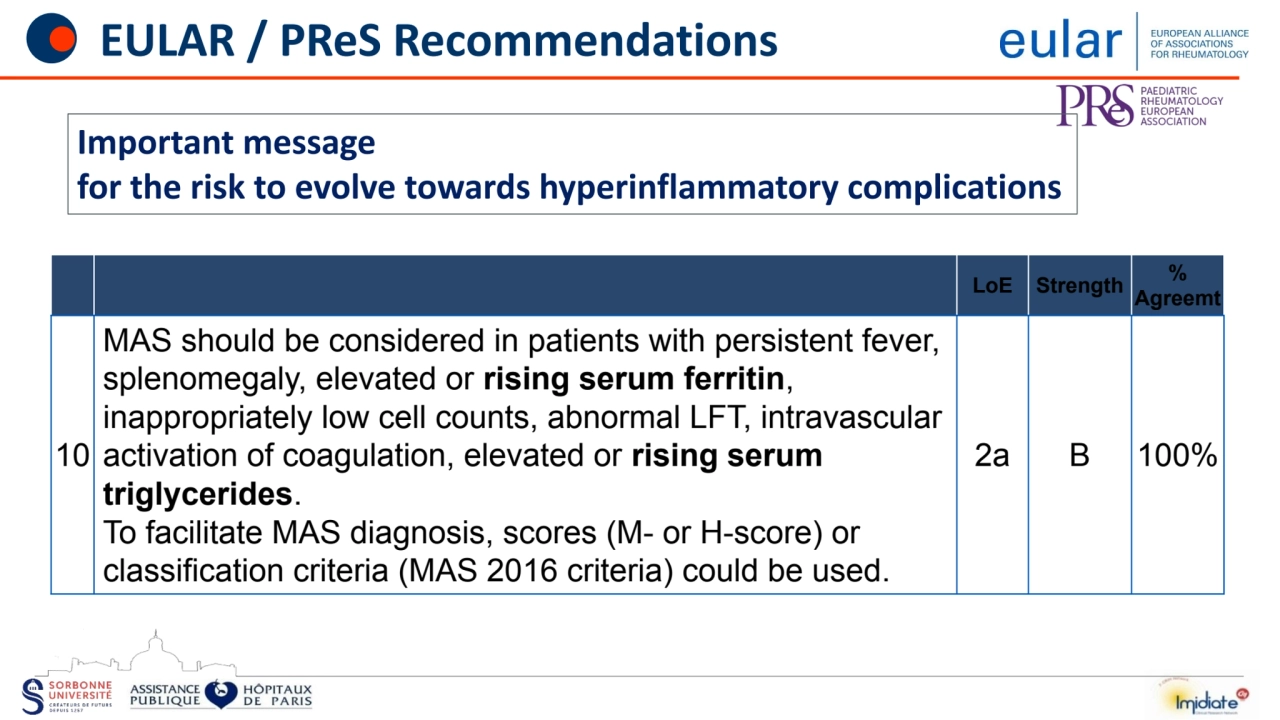
- 6. EULAR / PReS Recommendations LoE Strength % Agreemt 10 MAS should be considered in patients with persistent fever, splenomegaly, elevated or rising serum ferritin, inappropriately low cell counts, abnormal LFT, intravascular activation of coagulation, elevated or rising serum triglycerides. To facilitate MAS diagnosis, scores (M- or H-score) or classification criteria (MAS 2016 criteria) could be used. 2a B 100% Important message for the risk to evolve towards hyperinflammatory complications
- 7. For non-inflammatory D2T patients Patient living with Still’s disease
- 8. Conclusion
- 9. Conclusion EULAR / PReS Recommendations LoE Strength % Agreemt 14 Difficult-to-treat patients, those with severe MAS and those with LD should be managed in collaboration with Still’s disease expert centers. 5 D 96%
- 10. Thank you • Merci!