NextGen 2024: Unmet Needs & Clinical Trial Challenges Session Part 1
 AI Summary
AI Summary
Key Insights
- Around 20% of SJIA patients develop a refractory disease course despite IL-1 and IL-6 blocking agents.
- Refractory SJIA can present with different clinical patterns, including relapsing MAS, which may involve liver involvement.
- Patients with SJIA and relapsing MAS appear to be at risk for SJIA-associated lung disease.
- Liver biopsies of patients with SJIA and relapsing MAS often show elevated liver enzymes and characteristic inflammatory infiltrates.
- Challenges in clinical trials for smoldering MAS include not fully meeting criteria for MAS and difficulties with eligibility due to systemic features or background medications.
NextGen 2024: Unmet Needs & Clinical Trial Challenges Session Part 1
- 1. SJIA with relapsing MAS Alexei Grom, MD Cincinnati Children's Hospital Medical Center NextGen Therapies in SJIA, Still’s & MAS Washington DC November 13-15
- 2. SJIA with refractory course • Despite recently approved IL-1 and IL-6 blocking agents, about 20% of patients with SJIA develop a refractory disease course • fail to respond to all the approved biologic and non-biologic DMARDs • persistent disease activity requiring maintenance therapy with glucocorticoids • Several distinct clinical patterns of refractory disease • Refractory SJIA with predominantly persistent arthritis • Refractory SJIA with predominantly systemic features • SJIA with chronic parenchymal lung disease • SJIA with relapsing MAS • Includes a subgroup with predominantly liver involvement • Most of these patients do not meet eligibility criteria in the ongoing clinical trials in SJIA Erkens et al, Rheum Dis Clin North Am 2021;47:585
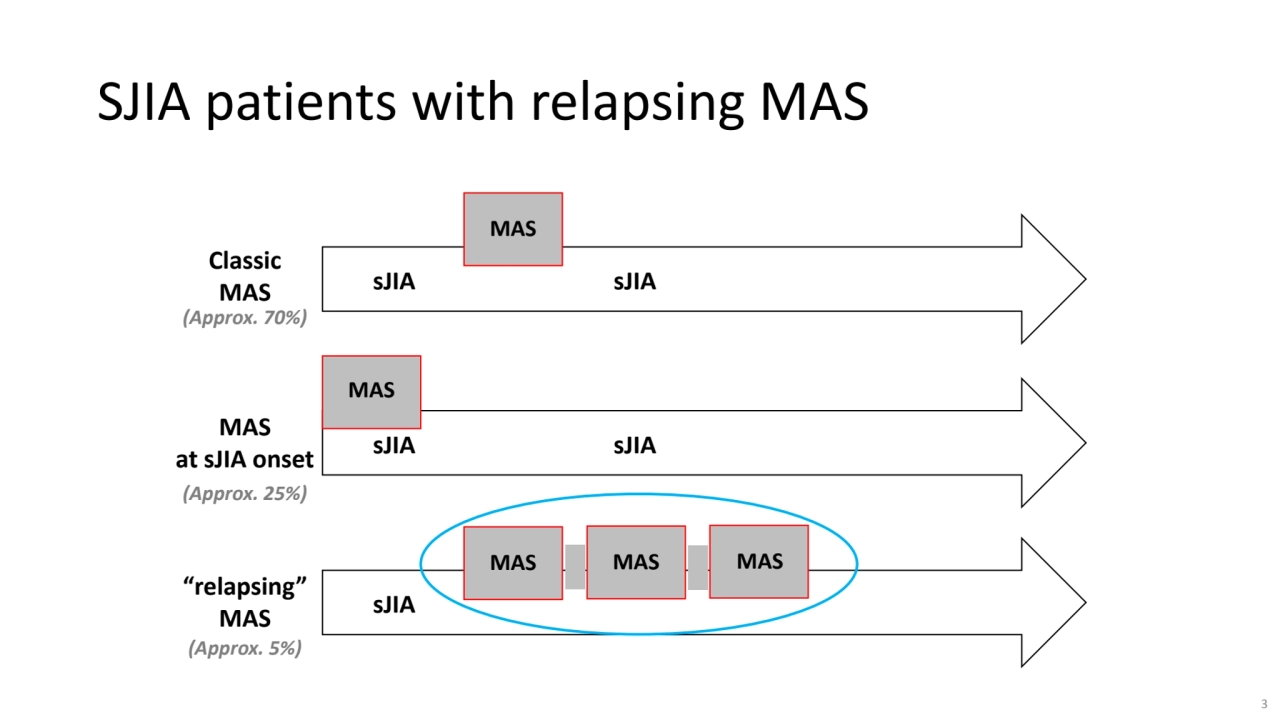
- 3. sJIA sJIA MAS sJIA sJIA MAS sJIA MAS MAS MAS Classic MAS MAS at sJIA onset “relapsing” MAS (Approx. 70%) (Approx. 25%) (Approx. 5%) SJIA patients with relapsing MAS 3
- 4. SJIA patients with relapsing MAS • These patients appear at risk for sJIA-associated lung disease • A large proportion of these patients have predominantly liver involvement 4
- 5. SJIA with relapsing MAS with Predominantly Liver Involvement • Persistently elevated liver enzymes with lab features of subclinical MAS (but do not meet full criteria for MAS) • Highly characteristic findings in liver biopsy − Sinusoidal inflammatory infiltrate that consists both of increased number of T lymphocytes and CD163+ macrophages − Highly activated Kupffer cells with some of them exhibiting hemophagocytic activity − Marked predominance of CD8+ T cells of CD4+ − Immunostaining for cytokines identifies CD8+ T cells as the main producers of large amounts of IFNγ • May have normal bone marrow biopsy • Increased serum levels of CXCL9 suggestive of high INF-γ activity in tissues
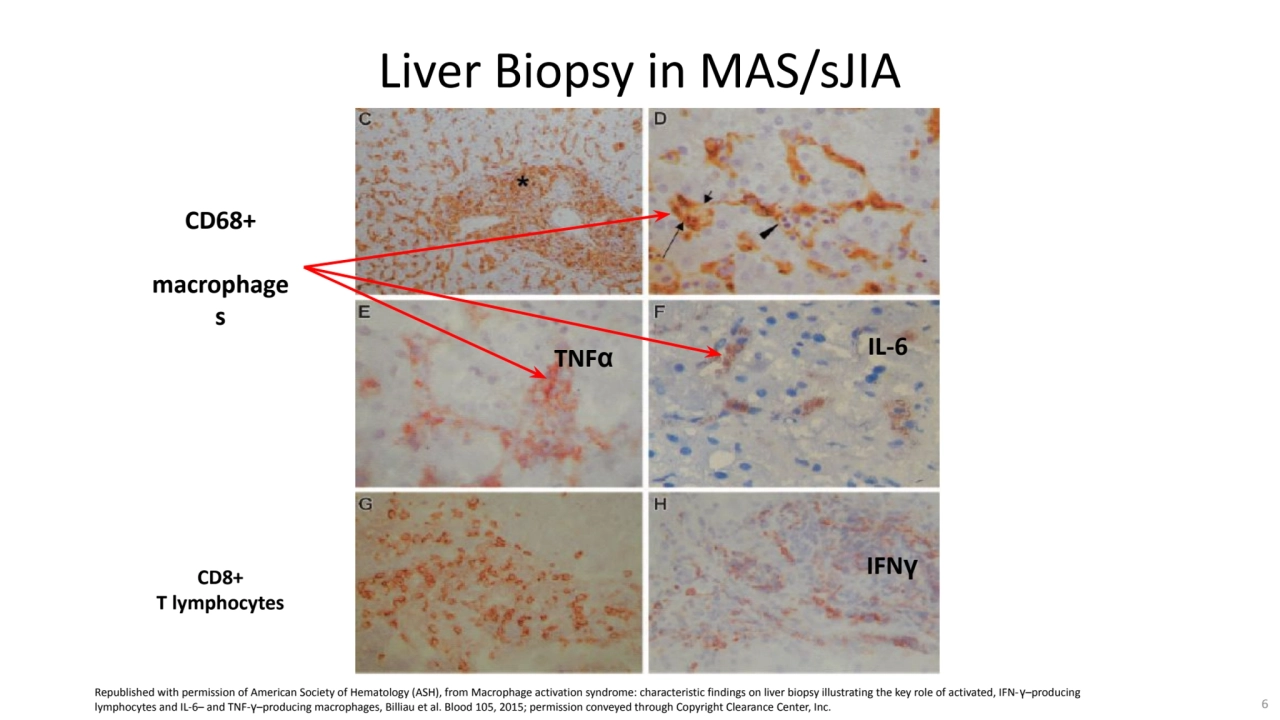
- 6. CD68+ macrophage s TNFα IL-6 IFNγ Liver Biopsy in MAS/sJIA CD8+ T lymphocytes Republished with permission of American Society of Hematology (ASH), from Macrophage activation syndrome: characteristic findings on liver biopsy illustrating the key role of activated, IFN-γ–producing lymphocytes and IL-6– and TNF-γ–producing macrophages, Billiau et al. Blood 105, 2015; permission conveyed through Copyright Clearance Center, Inc. 6
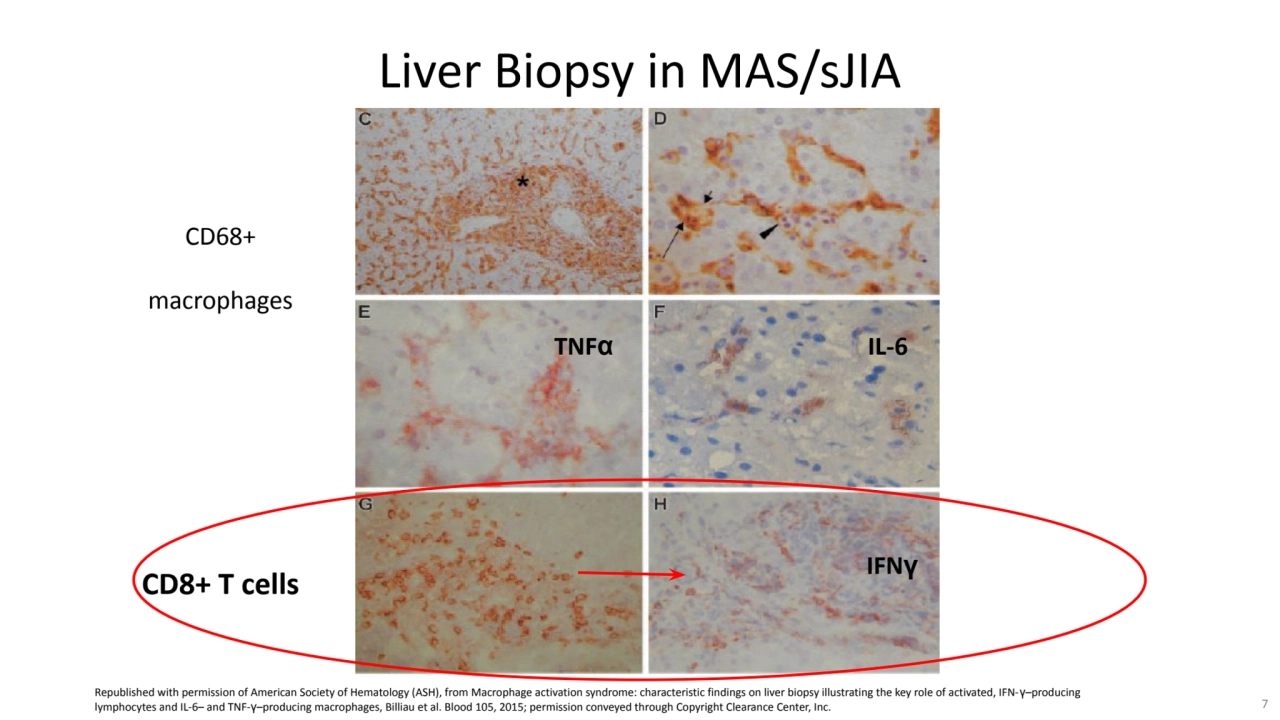
- 7. CD68+ macrophages Liver Biopsy in MAS/sJIA CD8+ T cells TNFα IL-6 IFNγ Republished with permission of American Society of Hematology (ASH), from Macrophage activation syndrome: characteristic findings on liver biopsy illustrating the key role of activated, IFN-γ–producing lymphocytes and IL-6– and TNF-γ–producing macrophages, Billiau et al. Blood 105, 2015; permission conveyed through Copyright Clearance Center, Inc. 7
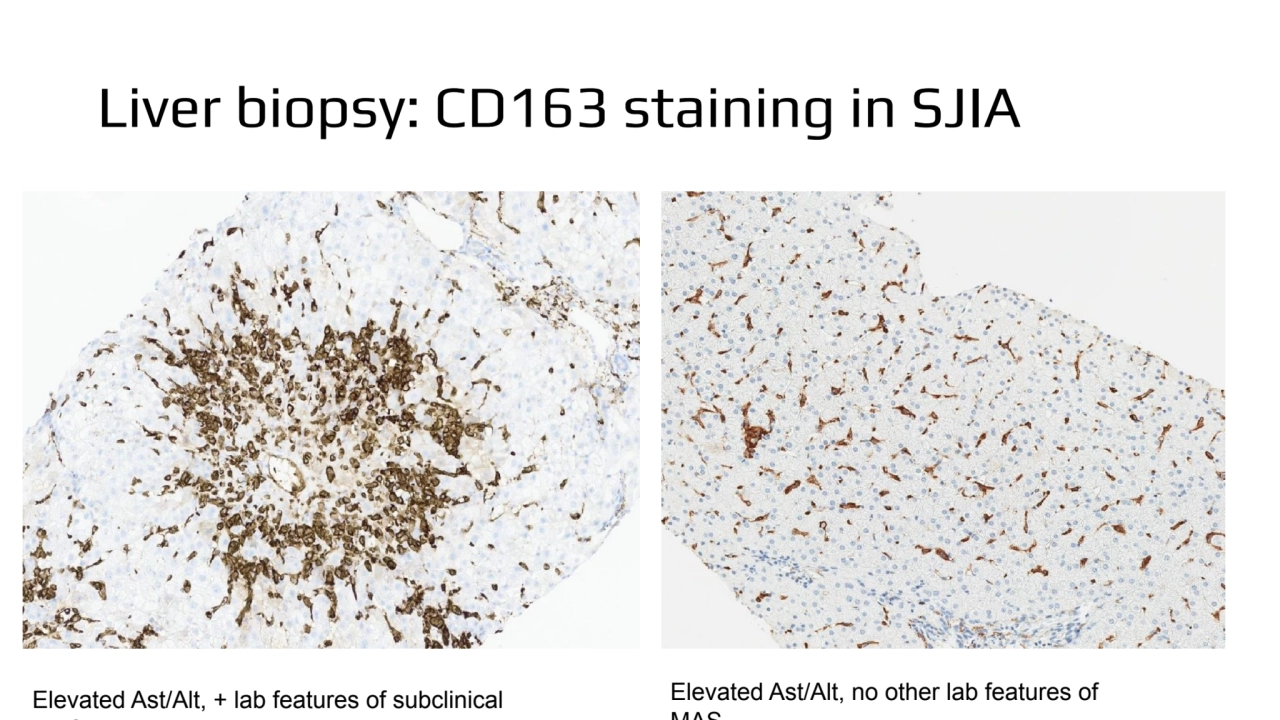
- 8. Liver biopsy: CD163 staining in SJIA Elevated Ast/Alt, + lab features of subclinical MAS Elevated Ast/Alt, no other lab features of MAS
- 9. MAS with Predominantly Liver Involvement • Similar histologic pattern observed by Prencipe et al. in 3 patients (2 of whom fully met the ILAR criteria for sJIA): − Large numbers of portal/periportal CD68+ macrophages and T cells • Liver biopsies showed highly increased levels of mRNA for IFNγ-induced genes, while other classical pro-inflammatory cytokines IL-18, IL-6 and TNFα were not markedly increased − Type I IFN induced gene expression was also roughly normal Prencipe G et al. PLoS One 2019;14:e0226043. 9
- 10. MAS with Predominantly Liver Involvement •JAKi? • CyA? • MMF? • Emapalumab?
- 11. Challenges with clinical trials in ‘smoldering MAS” • Do not fully meet criteria for MAS • Not eligible for MAS trials • If predominantly systemic features • Due to the absence of arthritis cannot be dx as SJIA and are not eligible for ongoing SJIA trails • Due to the absence of genetic dx, cannot be enrolled in the ongoing trials in inflammasopathies (such as anti-IL18/IL1 therapeutics in NLRC4 GoF) • Outcome measures for systemic aspect of the disease are not well defined • Options are modifying ACR JIA measures, or using Autoinflammatory Disease Activity Index, or Systemic JADAS • No clear how to handle numerous background medications (most trials require withdrawal with variable washout periods)